There are thousands of books on how to work with your abdominal muscles and which are the best exercises for them. However, only properly educated physiotherapists or trainers should give exercises for the abdominal exercises to people, especially when they are recovering from an injury or a disease.
This article is not about showing more types of exercises, but about explaining how a proper sit up exercise should be performed.
With the body in supine position, 3 major points are about to be analyzed: 1. flexion of the thoracic level, 2. flexion of the knees, 3. reciprocal inhibition of the iliopsoas muscle.
A little bit of anatomy
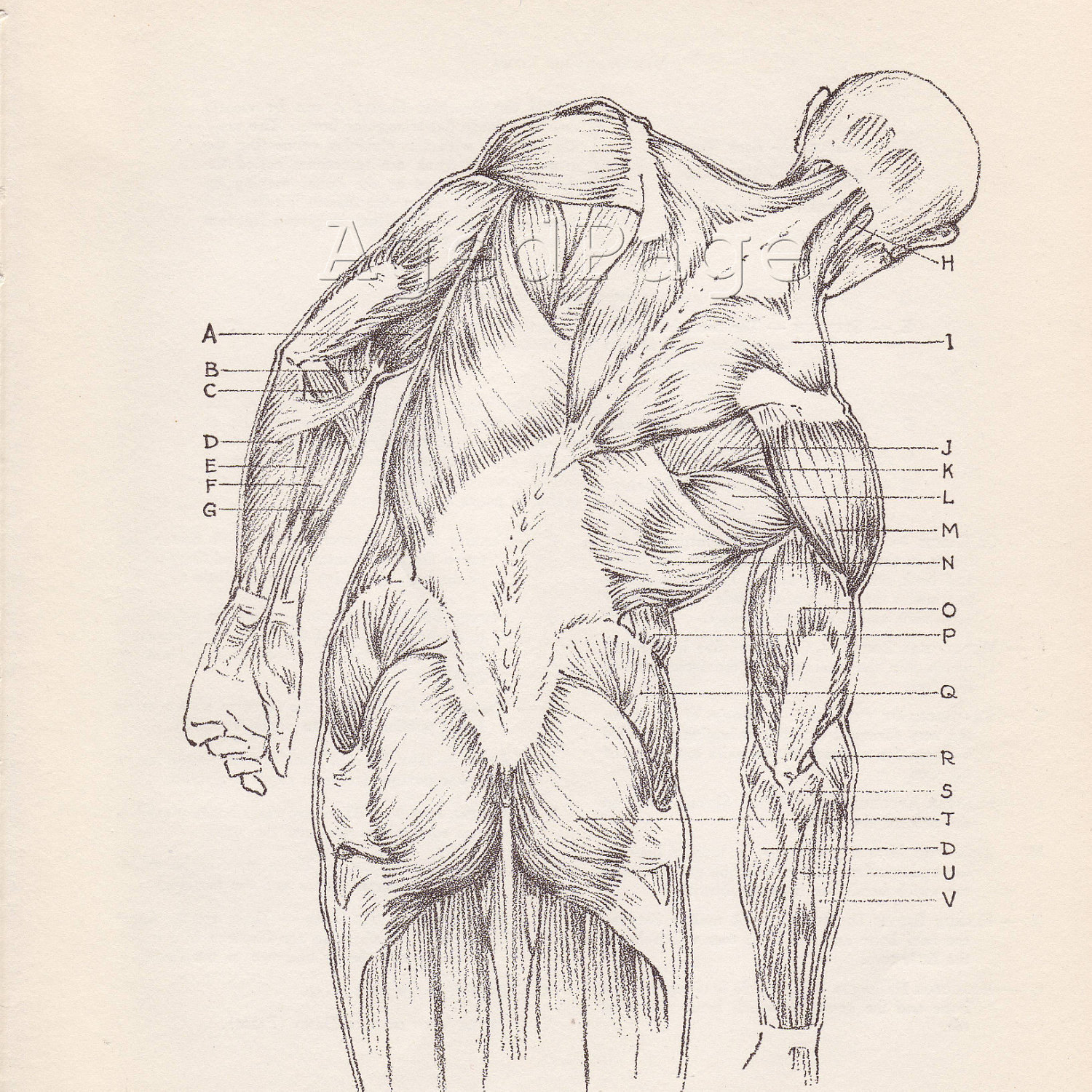
It is important for us to realize the origin and insertion of all our abdominal muscles - the obliquus externus, the obliquus internus, the transversus abdominis, the rectus abdominis, and the quadratus lumborum (I am not mentioning the pyramidalis, since it does not play a major role in the flexion of the rest of the abdominal muscles).
In the picture above, we cannot see the quadratus lumborum, but this muscle is very deep in the abdominal wall, originating from crista iliaca and inserting to rib 12, and process costalis of L1-L4 vertebrae. You can find more on that in your anatomy book.
The main function of the abdominal muscles is a. the flexion (forward bending) of the trunk against the gravity in the standing posture (our legs fixed) or b. the flexion of our hips in the hanging posture (our trunk fixed). It is very important to realize this "against the gravity" note, because a lot of people thing that when we bend forward while in standing position we use our abdominal muscles, which is not true. When we bend forward while in standing position, it is the gravity that is creating this movement and the back muscles that are activated eccentrically that hold us from falling down.
So, we can understand, that the only way to work with our abdominal muscles is by laying down and start lifting up our trunk with our abdominal muscles against the gravity.
There are also other muscles with the same function - the iliopsoas and the rectus femoris.
It is very important to understand that these muscles are also flexing our trunk (with legs fixed) or flexing our hips (with trunk fixed), because we need to inactivate them and isolate the abdominal muscles when we do the sit ups. In other words, we must be careful when we do sit ups not to work with our iliopsoas or our rectus femoris instead of the abdominal muscles due to wrong posture.
But how we can properly do that? Is it right to lay down completely straight and start doing sit ups? Should we bend our knees? Why? Would it be better to lift them up, above our pelvis? Why? Should we better ask someone to hold our feet on the ground? Or should we better ask him to pull our heels against us while we do the sit up?
Let's try to answer these questions.
In doing the sit ups, as we saw before, we need the isolate the abdominal muscles from the iliopsoas and the rectus femoris. And there are 3 completely safe ways to do that, that every physiotherapist and trainer should be aware of:
1. Flexion of the thoracic level
While doing the sit ups, we should flex only the trunk till the thoracic level, without lifting up the lumbar spine. This way, the abdominal muscles are activated completely. If we try to lift up the lumbar spine, then the iliopsoas is activated and is putting a lot of pressure on the lumbar spine vertebrae, which is quite dangerous, especially in patients with untrained abdominal muscles.
2. Flexion of the knees
By flexing the knees, we bring the biggest percentage of your center of mass above your pelvis or better, above the axis of rotation for the flexion movements of the abdominal muscles. This way, our muscles in the rest of the body are relaxed since we are not trying to hold our legs down on the ground, which we would try to do if we had our legs straight and the center of mass under the axis of rotation for the sit ups. Also, in this posture we rest the lumbar spine my flattening the normal lordosis and putting less pressure on the inter-vertebral disc.
What we must try to do during the sit ups is to inactivate the iliopsoas and the rectus femoris. There are 2 ways to do that:
a. lifting up the legs from the ground. This way, the iliopsoas and the rectus femoris are "loosing" their fixed point (the ground) and they are completely inactivated.
b. bend our knees, keep touching the ground while asking from someone to pull (and NOT hold on the ground) our heels towards him. This way, the gastrocnemius and the hamstrings become active and the iliopsoas and rectus femoris become inactive due to the
reciprocal inhibition effect.
So, next time someone asks you to hold his/her feet on the ground while he/she is doing sit ups, do NOT do it :-)










_en.jpg)